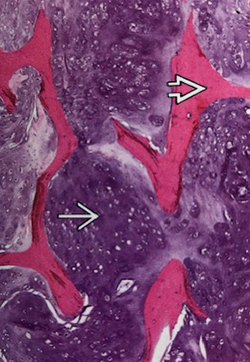
Chondrosarcoma
Chondrosarcoma is a malignant cartilage producing tumor of bone, the second most common after osteosarcoma.
Orthopaedic Oncology Service
Mass General - Boston
55 Fruit Street
Yawkey Building, Suite 3B
Boston,
MA
02114
Phone: 617-724-3700
Fax: 617-726-6823
Explore Chondrosarcoma*


Overview for Chondrosarcoma:
- Conventional chondrosarcoma accounts for greater than 90% of all chondrosarcomas
- Primary chondrosarcoma arises in normal bone
- Secondary chondrosarcomas arise in association with a pre-existing benign cartilage bone tumor, such as:
- Enchondromas have a very low risk of malignant transformation, (<1%)
- Conditions such as enchondromatosis/Olliers disease or Maffucci syndrome have a greater risk of malignant transformation, 35-40%
- Osteochondromas have a 5-25% risk
- They can arise in any bone, but most originate in the pelvis (especially the ilium) followed by the top end (proximal) of the femur and humerus, bottom end (distal) of the femur and ribs
- Infrequently develops in the small bones of the hands and feet (1%)
- Can occur in the cranium, usually the skull base
Presentation
- Pain, enlarging mass, limited range of motion (ROM), sometimes a fracture, and may be present for a long time
- Skull base tumors cause headache, double vision and weakness of the cranial nerves (nerves in the back of your brain, which send signals between your brain, face, neck and torso)
- Benign cartilage tumors, which begin to increase in size
Imaging
- X-rays show a lesion with defined borders that may contain popcorn, spotty or ring-and-arc calcifications, which are characteristics of cartilage tumors
- High-grade tumors usually have areas of cortical destruction (fractures) with a large soft tissue mass
- Additional imaging with MRI or CT helps identify extent of the tumor
- A bone scan shows significant uptake of the contrast dye
Determining Diagnosis:
- Bone biopsy with conscious sedation done by our musculoskeletal radiologist.
- Initial staging scans (e.g. bone scan, chest CT, MRI) to determine if the disease is localized or has spread (metastasized).
- Our sarcoma pathologists confirm diagnosis, which may take up to 1-2 weeks due to the specialized testing of tissue. Malignant bone tumors are graded 1 (low), 2 (intermediate), 3 (high), depending on how aggressive the tumor is.
Treatment:
- Almost entirely surgical.
- Aggressive curettage (scoop out the bone lesion and pack with cement) is done for low grade (1/3) chondrosarcomas, especially if the tumor is located in the extremities.
- High grade chondrosarcomas (3/3) require wide surgical resection with reconstruction.
- Chondrosarcomas arising in the pelvis are treated with resection regardless of grade because local recurrence in this region is very difficult to treat.
- Radiation has been used to treat unresectable tumors, and frequently used for tumors arising in the spine or skull base.
- Chemotherapy is not used for low grade chondrosarcoma because it has not been shown to help improve survival. Dedifferentiated chondrosarcoma may be treated with some of the same chemotherapy drugs that are used for osteosarcoma.
- Surveillance: After the initial postop visits (typically at 2 and 6 weeks), routine surveillance is for 10 years with imaging:
- Every 3 months for 2 years
- Then every 6 months for 3 years, which equals 5 years of follow-up
- Annual visit thereafter for 5 more years, which concludes the surveillance standard of care of 10 years (but most patients like to continue with an annual visit)
Orthopaedic Oncology Service
As members of the Cancer Center, our Orthopaedic Oncology team provides compassionate care to children, adolescents and adults with primary bone and soft tissue tumors (benign and malignant) and metastatic disease.